
In Clinical
Follow this topic
Bookmark
Record learning outcomes
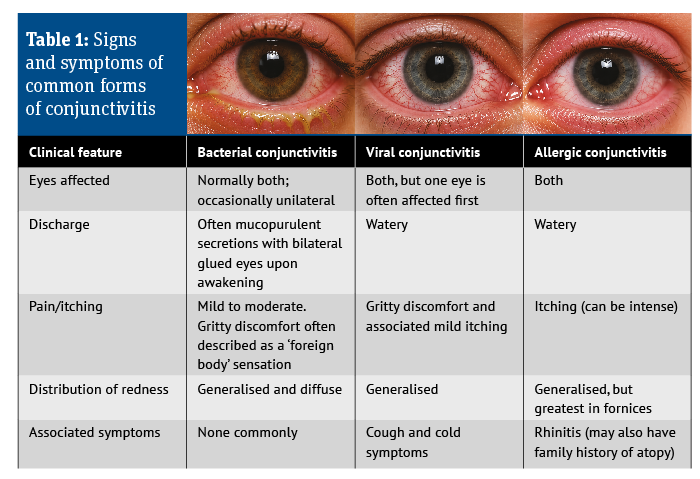
The causes of red eye seen most often in primary care are the different forms of conjunctivitis, characterised by varying degrees of ocular redness, irritation, itching and discharge. These presentations will be familiar to community pharmacists but are not the main focus of this article (Table 1 below summarises their key presenting features). Instead, let us examine some other scenarios, starting with diagnosis.
Establishing a diagnosis
Although conjunctivitis is the most prevalent cause of red eye, a detailed history and eye examination are essential to ensure that potentially sight-threatening causes are not missed. The history should include:
- Onset and duration of symptoms
- Severity and nature of discomfort
- Unilateral or bilateral presentation
- Presence of discharge
- Changes in vision
- Use of contact lenses or recent trauma
- Relevant family or medical history.
Examining the eye
A basic eye examination should always be performed. This can easily be undertaken in a pharmacy and does not require sophisticated or specialised equipment. A pen torch and reading material are usually sufficient. The eye examination will allow you to:
- Check pupil size, symmetry and reaction to light
- Assess the distribution of redness
- Identify the nature of any discharge
- Determine whether there is eyelid involvement
- Observe incidental non-red eye pathology (e.g. pingueculae, pterygium and xanthelasma).
Three basic steps should be undertaken; the order is unimportant provided they are all completed:
- Inspect the eye
- Check the pupils and reaction to light
- Assess reading ability.
Initiating the procedure
Explain the procedure to the patient and obtain consent. Wash your hands before the examination and position the patient so the eyes can be inspected. This is most easily achieved by asking the patient to sit down so that you are both at eye level.
Inspecting the eye
To fully assess eye redness, all aspects of the sclera should be examined. This is achieved through gentle manipulation of the eyelids. To examine the lower sclera, gently pull down the lower lid and ask the patient to look upwards, then to the left and right.
To examine the upper sclera, gently lift the upper lid and ask the patient to look downwards, then to the left and right. This process also allows observation of any discharge and assessment of eyelid involvement.
Checking pupils and reaction to light
Assessing the size, shape and reaction of the pupils to light can help identify potentially serious pathology. Conditions suitable for management within community pharmacy will generally present with pupils that are round, symmetrical, equal in size and reactive to light.
Careful visual inspection should allow assessment of pupil size and shape. To test the pupillary light reflex, use a pen torch in an area away from strong ambient light, which can make pupil reactions difficult to observe.
Ask the patient to look directly at you while bringing the light source in from the side of the face. Shine the light onto the pupil for less than one second to evoke a response. Both direct and consensual responses should be checked.

Checking reading ability
Visual acuity is normally assessed by optometrists using a Snellen chart. Normal vision is considered to be 20/20, while worsening vision is indicated by a higher denominator (e.g. 20/40 or 20/100).
Although this is not always practical in a pharmacy setting, reduced eye charts or reading cards can be used instead. Alternatively, a rough assessment can be made by asking the patient to read text of varying sizes from approximately 35cm (an arm’s length) away.
Each eye should be tested separately while the other eye is occluded. If the patient normally wears distance spectacles, these should be worn during testing. Difficulty reading with the affected eye compared with the unaffected eye may indicate reduced visual acuity.
Conditions that can be managed in pharmacy
Subconjunctival haemorrhage
Subconjunctival haemorrhage occurs when a blood vessel ruptures beneath the conjunctiva.
A segment of the eye, or occasionally the whole eye, appears bright red. It often occurs spontaneously but may be precipitated by activites such as coughing, straining or lifting.
The sudden onset and striking appearance commonly prompt patients to seek advice quickly. There is no pain, and patients should be reassured that symptoms usually resolve spontaneously within 10-14 days without treatment.

Blepharitis
Blepharitis is typically bilateral and presents frequently in community pharmacy with irritation, itching and burning of the lid margins. These may appear red and inflamed, with excessive tearing and crusting or skin flakes around the eyelashes.
Symptoms are often worse in the morning; patients may report that their eyelids stick together on waking. Symptoms are commonly intermittent, with periods of exacerbation and remission over many years. The mean age of onset is around 50 years.
Treatment involves improving lid hygiene using a diluted solution of baby shampoo mixed with warm water (1:10) and applied to the eyelids using a cotton bud twice daily.
Episcleritis
The episclera lies beneath the conjunctiva and adjacent to the sclera. Inflammation of the episclera causes a segmental redness affecting only part of the eye. In most cases, only one eye is affected. The condition is usually painless, although a dull ache may occasionally be noticed by the patient. Episcleritis is more common in young women. It is self-limiting and does not usually require treatment, although symptoms may take 6-8 weeks to resolve.
Conditions requiring non-urgent GP referral
Entropion
Entropion is an inward turning of the eyelid margin. It may be unilateral or bilateral, with the lower eyelid most affected. The inward turning causes the eyelashes to rub against the cornea (trichiasis), leading to ocular irritation and conjunctival redness. A white mucoid discharge may also be present. It is most often seen in older adults. Surgical repair is usually required, although temporary taping of the lower lid to draw the eyelid margin away from the eye may provide short-term relief.
Ectropion
Ectropion occurs when the eyelid turns outward, exposing the conjunctiva and cornea. Patients commonly present with a persistently watering eye. Paradoxically, this can also lead to dryness because the eye is not adequately lubricated.
Requiring ophthalmological intervention
Chlamydial conjunctivitis
Chlamydial conjunctivitis usually presents with bilateral diffuse redness, a gritty sensation and mucopurulent discharge. It should be suspected in sexually active patients aged 15-35 years. Many patients will also have an associated genital infection, of which they may be unaware.
Chlamydia can also be transmitted from mother to baby during birth. Bilateral red eye with purulent discharge occurring within the first month of life requires same-day referral to exclude neonatal chlamydial conjunctivitis.
Contact lens-related acute red eye
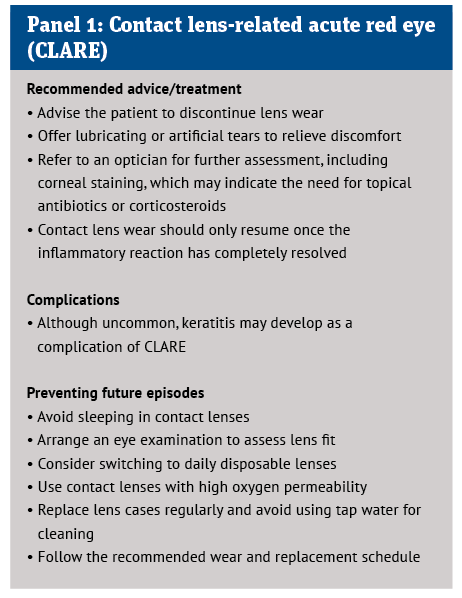
CLARE is a common but often overlooked condition that is most frequently seen in people who wear contact lenses overnight or for extended periods. Extended lens wear reduces oxygen supply to the cornea, creating a hypoxic environment that encourages bacterial growth, particularly gram-negative bacteria. This triggers inflammation of the cornea and conjunctiva.
Common symptoms include waking with a red eye, which may be particularly pronounced around the limbus, together with mild-to-moderate discomfort or pain, photophobia and excessive tearing. Same-day referral to an optician is required. Panel 1 outlines management.
Herpes simplex eye infection
Herpes simplex infection is commonly associated with cold sores and genital herpes, but it can also affect the eye. Symptoms include unilateral red eye, watery discharge, blurred vision, reduced visual acuity and eye pain.
Vesicular lesions may also be present along the lid margin or surrounding skin. Recurrence is common and corneal scarring may occur as a complication.
Conditions requiring urgent same-day referral
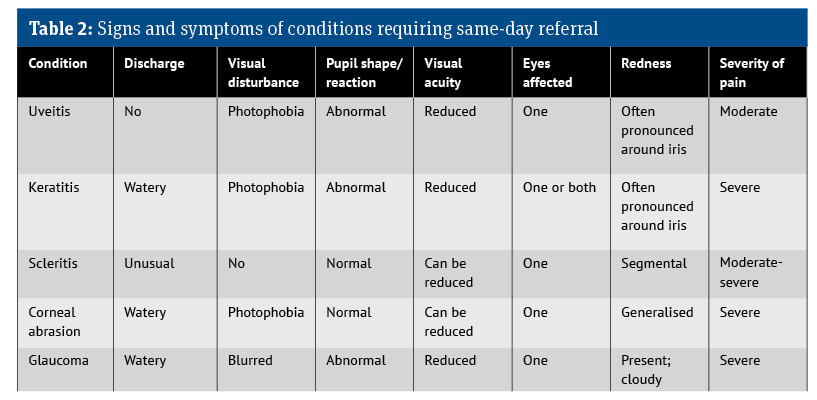
Five conditions that may present in community pharmacy – anterior uveitis, corneal abrasion, keratitis, scleritis and acute angle-closure glaucoma – can lead to sight-threatening complications. All are associated with true eye pain.
Table 2 summarises the signs and symptoms of these conditions, while Panel 2 highlights the features warranting same-day referral.
Anterior uveitis
Uveitis refers to inflammation of the uveal tract, which includes the iris, ciliary body and choroid. It is commonly associated with systemic autoimmune inflammatory disease, such as rheumatoid arthritis or ulcerative colitis.
Photophobia and pain are prominent symptoms, with the pain often described as a dull ache radiating to the brow or temple. Usually only one eye is affected, although bilateral cases can occur. Redness is often concentrated around the limbus, producing a ciliary flush.
On examination, the pupil may appear irregular, constricted or fixed, and visual acuity may be reduced. Pain may worsen during reading or close work. Immediate referral is required.
Corneal abrasion/foreign body
Corneal abrasions and foreign bodies result from trauma to the eye surface. Symptoms depend on the cause and severity of the injury. Common causes include fingernail scratches or accidental contact with sharp objects. Contact lens insertion and removal may also cause injury.
Patients may present with a red, watering eye accompanied by photophobia, severe pain and possible loss of visual acuity. Epithelial defects may be difficult to visualise with the naked eye but stain brightly with fluorescein and cobalt blue light.
Keratitis
Keratitis (corneal ulcer) is usually caused by infection. Severe pain is a prominent feature. Patients often also report photophobia, limbal flush, watery discharge and lid oedema. Examination may reveal reduced visual acuity, often accompanied by a constricted pupil.
Scleritis
Scleritis presents similarly to episcleritis, although pain – often severe – is a key distinguishing feature, together with blurred vision. Eye movement may exacerbate the pain. The condition is frequently associated with connective tissue disorders and autoimmune disease. For example, around 20% of affected patients have rheumatoid arthritis. Scleritis also tends to occur in older adults.
Acute angle-closure glaucoma
Acute angle-closure glaucoma often develops rapidly and usually occurs in the evening. The eye appears red and may look cloudy. Vision is blurred or reduced, and patients may report seeing haloes around lights. Severe unilateral eye pain, often associated with headache and vomiting, is typical. This is a medical emergency requiring immediate hospital referral.